Thalamic Neuron Theory: Theoretical Basis for the Role Played by the Central Nervous System (CNS) in the Causes and Cures of All Diseases
Abstract
Introduction
The general CNS (central nerve system) principle: all disease processes involve the CNS
The specific CNS principle: thalamic neuron theory
Principle of habituation or principle of "learning to be sick"
Principle of efferent control by the CNS
Principle of afferent control of the CNS or principle of physical neuromodulation
The principle of chemo-neuromodulation
Principle of dehabituation or principle of adynamic stat (principle of the stuck switch)
Principle of chemo-immuno-neuro-endocrino-modulation
Principle of bilaterality
Discussion, inferences, proposals and predictions
References
Abstract
The Thalamic Neuron Theory (TNT) postulates that the central nervous system (CNS) is involved in all disease processes, as the CNS not only processes incoming physical and chemical information from the periphery, it also sends out physiological commands to the periphery in order to maintain homeostasis for the entire body. Inherent in its capacity to learn and adapt (i.e. to habituate) is the CNS' ability to learn to be sick (pathological habituation) by looking in certain deranged central neural circuitries, leading to chronic disease states. These pathologically habituated states can be reversed by dehabituation through manipulation or modulation of the abnormal neural circuits by physical means (physical neuromodulation) like acupuncture, or chemical means (chemoneuromodulation) such as Chinese medicine, homeopathy or other modern medical techniques in a repetitious manner to mimic the habituation process. Chemoneuromodulation can also be achieved by delivery of minute amounts of pharmacological agents to specific sites in the periphery such as the acupuncture loci. It is hypothesized that humoral and neurotrophic factors and cytokines could be highly effective neuromodulating agents. TNT assumes the blue print for embryological development is embodied in the phylogenetically ancient part of the brain. This primordial master plan, organized in the form of a homunculus, possibly encased in a small nucleus, retains control over the subsequently evolved parts of the brain so that the entire CNS functions like a composite homunculus which controls the physiological functions of the entire body. TNT further postulates that the master homunculus takes the shape of a curled up embryo with its large head buried close to its pelvic region, with its large feet and hands crossed over to the contralateral sides. Neuronal clusters along a neuronal chain in the homunculus represent acupuncture points in the periphery. The neuronal chain itself represents a meridian and Chi is nothing more than the phenomenon of neurotransmissions. Certain new theoretical concepts such as the principles of Adynamic Stat and Bilaterality are also presented. Many difficult to explain clinical observations in modern medicine, Chinese herbal medicine, acupuncture and homeopathy can now be adequately explained using TNT. Based on this model, new therapeutic techniques can be launched to combat a whole host of intractable diseases.
INTRODUCTION
Notwithstanding the extensive modern therapeutic armamentarium, treatments of many important diseases are largely palliative rather than curative. This is so because the disease processes themselves are poorly understood. Even the cure of infectious diseases with antibiotics must rely on the ultimate defense mechanisms of the host. On the other hand, reported successes of herbal medicine, acupuncture, and homeopathy have been largely discounted as unscientific, simply because no explanation has been offered by modern medical sciences. But what if the efficacy of these unconventional therapies is real? The author believes the answer is already available, camouflaged. among known scientific facts, but somehow fails to be recognized. A hypothesis, tentatively named 'Thalamic Neuron Theory', using the known elements of scientific facts as its building blocks, is hereby proposed to explain the causes and cures of all diseases. This hypotheses consists of nine primary principles:
The general CNS (central nerve system) principle: all disease processes involve the CNS
Modern medical texts rank the entire nervous system as the equivalent of any other system, be it cardiovascular, digestive or musculoskeletal, etc. The nervous system, especially the central nervous system has never been thought of as the master system of all others, as it should be. Furthermore, the body is viewed as a machine with various parts functioning autonomously without close relationships with one another. Even as the cellular and molecular events have been analyzed in great detail, such knowledge has not been fully integrated for the whole functioning organism. It is only relatively recently that the mind is popularly believed to have the ability to cause illnesses as well as to modify disease processes, including the process of healing.
Intuitively; it seems unthinkable that with the myriads of bodily functions to be monitored and the multitude of biochemical reactions taking place all over the body, there is no higher control by the CNS. If one should subscribe to this notion of highly organized control by the CNS, then one must inevitably conclude that every malfunction in the periphery (in contrast to the CNS) must be sensed by the CNS in order that corrective measures be taken. This sensing or recognition of the disturbance in the periphery by the CNS must be translated into changes in the neural circuitry within the CNS responsible for the disturbed physiological function. Based on this simple premise, the following inferences may be made:
-
Every dysfunction arising from the periphery, be it a burn injury to the right forearm, an infection caused by invasion of streptococci in the pharynx or an ingestion of toxic substances into the stomach, will either immediately or eventually lead to an equivalent derangement in the equivalent neural circuitries within the CNS.
-
The CNS then responds by instituting corrective measures, resulting in the normalization of these neural circuits which then correct the deficiencies in the diseased part of the periphery to end the disease process.
-
If the normalization of the physiological programs embodied in the neural circuitries in the CNS is impaired, the initial derangement may remain status quo or can cause other neural circuits to go awry. Hence the disease either stays chronic or progresses.
-
Any event that can adversely affect any central circuitry is therefore capable of inducing pathological changes, resulting in diseases. Overly intense emotions such as anger, grief or fear can cause the central circuitries to malfunction. A case in point is the clinical findings associated with post-traumatic syndrome in US servicemen in the Vietnam war era. Likewise, devastatingly strong physical stresses such as excessive heat, cold, humidity, etc. are equally capable of setting up neurophysiological derangements within the CNS. These resultant malfunctions in the CNS can not only themselves cause physical illnesses, but can also set up such conditions as to increase the individual's susceptibility to other pathogenic processes. Conceptually, traditional Chinese medicine places great emphasis on the ability of physical and mental stresses to cause diseases, as its principles are based on functions and behaviors of the central nervous system (according to this hypothesis). On the other hand, modern medicine until recently has failed to recognize the disease causing potential of purely emotional and physical factors as it has failed concurrently to recognize the controlling roles played by the CNS.
-
The CNS itself can also malfunction due to aberrant biochemical reactions stemming from say, genetic diseases like manic depression, Huntington's chorea, etc.
The general CNS principle states that the CNS is universally involved in all diseases, regardless of whether they originally arise from the periphery or are indigenous to the central nervous system; whether initiated by various infective agents, be it viral, bacterial, rickettsial or parasitical in nature or resulted from exposures to toxins, radiation, physical injuries, or emotional upheavals. Frequently, long after the culpable causative agent has been eliminated following the injurious insult to the host, the resulting dysfunction-ing central circuitry nonetheless persists and chronic disease ensues. The importance of this concept is no matter whether the CNS is the culprit or victim, that is, whether it is the initiator or the receiver of the noxious event, it may now have become the focus or cradle of pathological processes which continue to affect the peripheral functions adversely. By the mere recognition of the role the CNS plays in all diseases, in conjunction with the principles to follow, much clinical data will begin to make sense. Recognizing the CNS as the missing link, giant steps can be made to resolve a great number of difficult clinical problems.
The specific CNS principle: thalamic neuron theory
While the first principle may prompt the medical profession to look at diseases in general in a totally different light, it lacks specifics in the elucidation of the neurophysiological mechanisms through which practical clinical benefits may be derived.
Therefore, thalamic neuron theory (TNT), first proposed in 1977 (1) to explain phenomena relating to pain, is now modified and expanded to include all other disease states:
Central representation by homunculus
Since the CNS not only processes all information coming from the periphery (the entire body including the brain itself), but also sends out commands to the periphery to institute maintenance and corrective functions, this central control must be highly organized. As each part of the periphery must be represented centrally, it is only logical to infer that the entire body should be represented as a miniature human body or homunculus. This is hardly a new revelation because decades ago Hassler mapped a homunculus in the sensory thalamus in man by observing the unpleasant tingling effect in various parts of the body elicited by stimulation of thalamic sites in the course of stereotaxic surgery (2).
Multiple connecting homunculi
If a homunculus subserves one or more physiological functions, be it sensory or motor, or whether it has to do with proprioception or smooth muscle contractions, it must communicate with other homunculi for different functions in order to process the vital information and initiate appropriate signals or commands to the periphery. Therefore the various homuncull would have to be integrated. In other words, the joint functions of these connecting or communicating homunculi can be viewed as a composite homunculus summarizing their total actions.
Organization of the composite homunculus
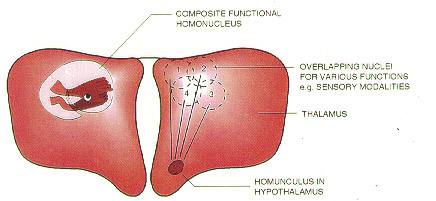
Functionally, the composite homunculus behaves as if it has taken the shape and posture of a primitive embryo with its large head buried close to its pelvic region, and its large feet and hands crowded together in the vicinity of the face but with both hands and feet crossed over the midline to the contralateral sides (Fig. 1). Along the longitudinal axis or the head to tail direction are neuronal chains forming pathways of facilitated neural transmissions with spontaneous sequential discharges and transmissions in a clockwork manner. The spatial arrangement of these neuronal chains within the composite homunculus follows that of the acupuncture meridians in the periphery. Also representing acupuncture loci in this homunculus are functionally discrete clusters of neurons along these pathways (meridians). These neuron clus-ters (central equivalent of acupuncture points) have extensive synaptic networks and thus have a much greater sphere of influence than other neurons in the homunculus (Fig. 1).
At least one master homunculus
In order for the composite homunculus to behave in ways just described, there must be at least one master homunculus organized spatially in such a manner to integrate the other homunculi (Fig. 2). It must also maintain close connections with, and possess the ability to influence the other homunculi. In other words, many of the homunculi may or may not have the fetal posture or spatial arrangement, yet if they are in close communication (i.e. hand to hand, chin to chin, etc. from one homunculus to the master homunculus) with the master homunculus which is organized as a curled up fetus, then the functional phenomena that emerge after processing by the master homunculus will be exactly the same as those of a composite homunculus having such spatial arrangements.
Hierarchy of the brain
Phylogenetically older parts of the brain such as the thalamus and hypothalamus should claim supremacy over the evolutionarily newer parts of the brain. This does not down play the importance of the neocortex, it simply says the primordial part of the brain is still the prime mover which controls the most essentialphysiological functions. It is likely that the master homunculus or mini brain is located somewhere in these ancient parts of the CNS.
Armed with this specific CNS principle, attempts can now be made to interpret some of the most fundamental concepts in traditional Chinese medicine that have been most difficult to understand from the modern scientific viewpoint:
Meridians exist only in the brain. According to this hypothesis, the meridians do not exist in the periphery; rather it is buried deep in the CNS. The nerve endings along the imaginary lines on the surface of the body known as the meridians do, however, project onto and connect with the neuronal chains within the homunculus (3). Chi is nothing more than neural transmissions (4). Since spontaneous neural discharges do occur along these meridian pathways centrally, they are equivalent to the flow of chi and can sometimes be felt subjectively as a sensation travelling along these pathways on the body surface. On the other hand, stimulating nerve endings of an acupuncture point along a meridian at the periphery will ensure the stimulation be transmitted to the representing neurons in the homunculus along the neuronal chain that represents the meridian and so it is possible to induce a sensation travelling along the meridian in the periphery even though the sensation is felt inside the brain. It is therefore futile to try to look for an anatomical entity called meridian in the periphery, for it is merely a series of nerve endings at the periphery.
Referred pain and meridian. Furthermore, the pattern of referred pain often coincides with the distribution of the meridians rather than the segmental distribution of peripheral nerves. A hyperexcitable focus in the homunculus, equivalent to what is known as a trigger point in the periphery, when stimulated, can give rise to pain along the neuronal chain to cause pain at a distance, the so-called referred pain. Stimulation of acupuncture point also causes the neuronal activities in that whole region around the neuronal cluster to normalize and this is what imparts to the acupuncture loci their clinical efficacy.
Impeded neural transmission causes disease. According to the Chinese medical teachings, an impeded flow of chi caused by either congestion or deficiency along a certain meridian can cause both disease and pain. From the modern medical point of view, hyperfunctional or hypofunctional neurons along a neuronal chain prevent normal neural transmissions so that an abnormal focus is set up within the homunculus, causing disturbance in the homeostasis of the periphery. As a road block is set up along the neural transmission pathway, the subjective sensation of pain is often felt.
Clockwork neural transmission along the neuronal chains. More interestingly, the 12 traditional meridians, each connected to an internal organ and associated with a distinct symptom complex, are linked up with one another head to tail to form a great loop with the circulation of chi completing the entire loop in 24 h, activating a new meridian (segment of the great loop) every 2 h. This internal biological clock may in fact govern many of the circadian rhythms of the body's functions. A similar system may also exist in migratory birds as an instrument for navigation. It may also explain why symptoms vary in severity during the day, waxing and waning in a cyclical manner despite the lack of change in the disease process itself.
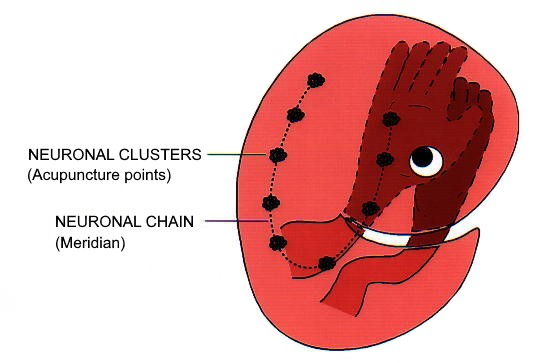
Fig. 1 A homunculus representing the entire body is hypothesized to exist somewhere in the CNS, particularly the phylogenetically ancient part of the CNS. Such a homunculus is organized in the shape of a curled up embryo with its large head buried close to the pelvic region and its large hands and feet crossed over the midline to the contralateral sides and crowded together in the region of the head. For the sake of clarity, only the right extremities are shown. A neuronal chain representing a meridian in the periphery is shown along with clusters of neurons which represent the acupuncture points. This model is extremely useful in explaining many acupuncture phenomena. For example, a point between the thumb and index finger known as the Ho-ku point is useful in the treatment of problems of the face because the treatment point is actually in close proximity to the face within the CNS.
Homunculus model as solution of therapeutic enigmas. While traditional medical principles have been faithfully followed, historically no one has come forth with adequate explanation for many of these principles. For instance, why should the famous Ho-Ku point between the thumb and the index finger be useful in the treatment of diseases of the face, or why should the Lin-Shi (Near Tearing) point between the fourth and fifth metatarsals of the foot be used to treat problems around the waist, or why a distal point on an extremity is used to treat a clinical condition
Fig. 2 The blue print for somatic development may be embodied in the phylogenetically ancient part of the brain which may also be the internal organization of neural tissue in early embryological development. Newer parts of the brain have been added as 'outgrowths' of this primordial brain in the course of evolution. The old blue print or master homunculus retains connections and control over the new additions. Even though nerve fibers of different sensory modalities projecting to different neuclei or structures in the thalamus may or may not have the embryonic spatial arrangement as depicted in Figure 1, but as long as they are inter-connected with and integrated by the master homunculus, the whole CNS can functionally behave as a composite homunculus having the special spatial arrangements as in Figure 1. The master homunculus may be found in the thalamus or elsewhere in the ancient portion of the brain including the hypothalamus.
on the contralateral side? Fortunately, the seemingly great distance between the point of treatment and the point of pathology disappears the instant we examine the embryo-shaped homunculus model (Fig. 1), as the points of treatment and points of pathology are actually in close proximity. Many of the anatomically baffling socalled convergence points can also be explained on this basis.
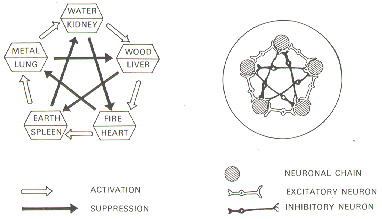
The five elements and the homunculus model The five elements and the homunculus model. The meridians, running along the longitudinal axis of the homunculus from head to extremities and vice versa, form a bundle shaped like a horse-shoe (Fig. 3). Additionally, each meridian is assigned a symbol of one of the five elements: metal, water, wood, fire and earth, bearing with one another a symmetrical relationship of activation and suppression (Fig. 4A). This apparent metaphysical denotation in actuality functions as a set of scientific symbols to designate the excitatory and inhibitory functions originating from one neuronal chain to another. Excitatory and inhibitory neurons are simply sandwiched between the neuronal chains within this bundle of neural transmission pathways equivalent to the meridians (5) (Fig. 4B).
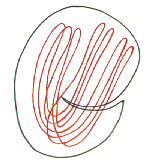
The rhythmic method and the spiral neural trans-mission pathway. A more sophisticated treatment method involves 66 acupuncture points below the knees and elbows. These points can be employed clinically
Fig. 3 A simplified schematic representation of the neuronal chain (meridians) in the homunculus. Meridians are hooked up head to tail in a continuous loop which then folded upon itself into a horse-shoe shaped bundle with one limb of the bundle extending along the extremities and the other towards the head region.
according to a biorhythm that takes 10 days to complete (6). According to this method, certain points will 'open' at designated hours on specific days, and become super-effective when stimulated. From a modern scientific viewpoint, the opening is
Fig. 4 A side by side comparison of (A): the five elements along with diagrammatic illustration of the activation and suppression of rela-tionships among the five elements in traditional Chinese medicine and the organ systems they represent and (B): a simplified schematic representation of the cross section of the bundle of neuronal chains (meridians) along with the excitatory and inhibitory neurons sandwiched between them. These figures illustrate that the abstruse concept of the five elements can be quite simply explained by neurophysiological phenomena.
equivalent to a state of activation which makes it more effective in influencing other neurons. The pattern of opening can be shown to depend on another system of circulation of chi, or neural transmission along a diagonal spiral pathway connecting the different neuronal chains, with the activation hopping from one pathway to another in a cockscrew fashion (Fig. 5)
The building blocks of TNT, such as neuronal chains, neuronal clusters, excitatory and inhibitory pathways, homunculus, embryonic posture of the homunculus, etc. are nothing out of the ordinary, yet it is capable of explaining not one or two isolated Chinese medical principles, but the majority if not all of those principles, many of them have stumped physicians for centuries.
Principle of habituation or principle of "learning to be sick"
Basis of habituation
The classic experiment of conditional reflex by Pavlov shows that the gastric secretion of a dog can be induced by the ringing of a bell, only after
Fig. 5 A simplified schematic representation of the spiral neurotransmission pathway which primarily hops from one neuronal chain to the other in a diagonal and spiral fashion. This circulation of Chi or neurotransmission primarily involves the 66 points distal to the knees and elbows of the extremities.
peated sessions of feeding immediately following the ringing of the bell (7). More recently, Kandel was able to demonstrate that the gill withdrawal reflex in Aplysia to tactile stimulus will cease after repeated identical stimulations, implying the animal can learn and remember with its simple abdominal ganglion by readjusting the sensitivity of certain specific neurons (8). Simply put, learning has to do with the setting up of a circuitry within a neuronal structure which will respond quickly or automatically to an environmental stimulus previously experienced. These previous stimuli must be able to somehow change the excitability or sensitivity of the neurons in a specific neuronal pathway in order that facilitated transmission be activated promptly on demand. Learning, conditional reflex, habituation and memory are but the different expressions of the same basic phenomenon - the changing of the neuronal sensitivities to form a special circuit or program. Learning or habituation can be accomplished in to ways:
-
By frequent repeated stimulations: as in learning to play a piano or tennis by repeatedly activating the same neuromuscular elements which input information to the brain, a procedure we call 'practicing', or as in the memorization of a poem by repeated recitals, or in drug addiction by repeated chemical stimuli to the CNS with 'habit forming' substances like alcohol and heroin
-
By a single strong stimulation which may be overwhelming or traumatic in nature. In the latter case, a neural circuit can be said to have been 'shocked' into a state of habituation.
Habituation or learning as a disadvantage inherent in an advantage
While the nervous system's innate ability to learn allows an organism to quickly adapt to its environment, thereby enhancing its survival skill, this very same nervous system is also capable of learning 'bad' habits, deranging its central neural circuitries in such a way as to bring about permanent disabilities as in many chronic disease states. Such a nervous system is blessed and cursed at the same time. Blessed because it possesses the evolutionary advantage to adapt, and cursed because it can learn to be sick just as easily. The paradox is that the faults of the CNS are inherent in its advantages. But since the advantage for survival far outweighs the problems of an occasional sickness or disease which does not severely impair the species' ability to procreate, this imperfect system has been inherited by all living creatures today. It is therefore not necessarily 'survival of the fittest' as Darwin puts it, it is simply 'survival of the fit' without having to be the 'fittest'.
Habituation by repetitions
Cumulative micro-traumas from repetitive motions associated with various occupations have been the outstanding causes of many chronically painful conditions (9). Noted examples are tennis elbows, swimmer's shoulders, video gamer's fingers, butcher's wrist and the list goes on. Chronic hearing loss may indeed be a result of habituation. By getting 'used' to the loud ambient noise, the sensitivity of the central neurons serving the auditory function may be lowered in order to tolerate the excessive noise. When the lowering of the auditory acuity or hearing-stat is frequent and chronic, it may get 'stuck' at a low setting, thereby resulting in hearing loss. The development of myopia can be hypothesized to follow a similar pattern of habituation. The chronic repetitive eye strains, and the sustained accommodation efforts to permit the eyes to read or look at close-up objects get the visual apparatus stuck at the new setting for near vision.
Another classic example of pathological habituation can be found in an experiment in which squirrel monkeys are subjected to electrical shocks preceded by flashes of light. The shocks can be avoided if the light is turned off in time. The monkeys at first respond to the stressful task with transiently elevated blood pressures. But as the stressful situation continues, in anticipation of the shock, the mean arterial blood pressure goes up even before these training sessions. As this process is repeated continuously, the monkeys finally developed chronic hypertension (10,11). In other studies, long term high sodium diet can also cause high blood pressure (12,13). The possible mechanism of pathogenesis according to the present principle is as follows:
The high sodium content in the blood (hyperna-tremia) produces thirst which is followed by intake of water which in turn expands the intravascular volume. The crowding inside the vascular bed causes the blood pressure to be set high. If this diet is continued for a sufficiently long period, such repeated stimuli will compel the body to learn to keep the blood pressure at a high setting, so chronic hypertension ensues.
Habituation by 'traumatic' experience
Pathological habituation can also occur in one fell swoop. Traumatic insults to the central nervous system including severe noxious stimuli from the environment, such as extreme cold, heat, humidity, change in barometric pressure, chronic worrying, surge of strong emotions such as anger, fear, sadness, assault on the body by infective agents, etc. can all wreak havoc to the CNS by setting up abnormal circuitries. It is not uncommon that long after the initial precipitating illness has passed, a chronic state of pathology persists. In both syphilis and Chagas' disease (14) (caused by the parasite Trypanosoma cruzi), most of the tissue damages occur during the chronic phase when the infective agents are no longer present. The onset of rheumatic fever or glomerulonephritis occurs many days after an episode of streptococcal infection from which the host has already recovered (15). Insulin dependent diabetes mellitus can develop after mumps or congenital rubella (16,17). According to TNT, once the abnormal pathological focus is set up within the composite homunculus and its related parts in the brain, the process may continue indefinitely as a chronic illness.
Principle of habituation and ancient tenets
Surprisingly, the principle of habituation also provides the solution to puzzles contained in ancient authoritative medical text. For instance, in NeiChing or Yellow Emperor's Book on Internal Medicine, one can find the following passage in the chapter known as 'the Grand Thesis on the Phenomena of Yin and Yang'(18):
Injury by cold in winter inevitably causes febrile
illnesses in the spring; Injury by heat in summer
inevitably causes chilly illnesses in the fall.
Nei Ching to Chinese medicine is like the Bible to Christianity. However, no one has yet been able to decipher the true meaning of this abstruse tenet, although it is often used to help make diagnoses by. eliciting from the patient medical history of exposure to cold or heat. Nevertheless, the answer becomes apparent once the habituation principle is applied. When the body is subject to excessive cold, it will raise the metabolic rate to compensate for heat loss. Cold injury in this case thrusts the metabolism-stat to a higher setting where it gets stuck (habituation). Come spring time, a warmer environment normally signals the CNS to set the metabolism-stat at a lower point, but since the control is jarred at a higher range, the body becomes hypermetabolic in relation to the seasonal environment and is therefore predisposed to the development of febrile illnesses. The same reasoning can be applied to the remaining principle concerning injury by heat in summer.
Principle of efferent control by the CNS
Clinical facts and experimental data point to the inescapable conclusion that the CNS can and does control the various peripheral regions in many ways. Biofeedback experiments prove that conscious voluntary effort (emanating from the CNS of course) can change heart rate, galvanic skin resistance, skin temperature, etc. (19). Under hypnotic suggestion, blister can form on the skin of a subject by placing on it a warm coin (not hot enough to burn the skin) or touching it with a pencil while suggesting to the subject the coin or the pencil is red hot (20,21). In this instance, messages originating from the CNS markedly exaggerate the physiological response to a non-noxious stimulus. Stress ulcers in the stomach found in soldiers who died in active combat and gastric erosions occurred in rats subjected' to water immersion stress (22) prove unequivocally that physical and emotional stress can induce trophic changes in the viscera. That cardiac arrythmia can be found in patients suffering from strokes and chronic electrostimulation of the hypothalamus produces early atherogenic change in the aortas and coronary arteries of rats (23) attests to the fact that deranged central neural circuitries can cause dysfunctions in a peripheral organ and tissue. It has been recently reported that head injury can cause a whole host of complications relating to different organ systems such as consumption coagulopathy, electrolyte imbalances, neurogenic pulmonary edema, cardiovascular hyperdynamic state, stress gastritis, etc. (24). These well documented clinical phenomena are hardly sporadic and coincidental findings. The nervous system, doing much more than transmitting sensory information to the brain or effecting motor functions, actually controls the peripheral environment including its biomolecular environment. The ubiquity of nervous tissues (25) in the body supports the theory that their presence is to maintain homeostasis.
Having stated the facts above, a reasonable question to ask would be: can a focus of abnormality in the CNS such as a blockage in a certain part of the composite homunculus cause degenerative diseases including cancer in the peripheral part represented by this abnormal focus? A neuronal derangement in the homunculus can affect the peripheral equivalent part in two different ways. First, if the central abnormal focus is hyperactive, it may bombard the periphery with excessive chemical messages that change the local homeostasis radically, causing abnormal tropic changes. Or second, if the focus is hypoactive, the deficient communication with the periphery permits too much autonomy for the peripheral cells it normally controls to go haywire. Cells are equipped with all the available genes to allow them to differentiate. Normally, only the appropriate set of genes is activated. They are also equipped with the internal machinery to make different kinds of humoral factors including hormones as cancer cells have been found to produce substances like gastrin, antidiuretic hormone, parathyroid hormone, etc. (26-28). Such cancer cells are out of control with the wrong set of their genes turned on because the CNS has failed to suppress them due to the lack of controlling chemical messages. It appears both a deficiency and an abundance of chemical messages originating from the CNS can produce equally devastating results.
That cancer can cause pain is a well accepted notion, but can pain cause cancer? According to traditional Chinese medicine, chronic impedance of chi, equivalent to abnormal neural transmission within the composite homunculus, can lead to cancer or tumor. The same blockage also causes pain. So in reality blockage that causes pain is potentially carcinogenic under the right circumstances. And interestingly enough there is a significantly higher incidence of neoplasm among chronic pain sufferers than the general population.
Principle of afferent control of the CNS or principle of physical neuromodulation
So far, the thalamic neuron theory (TNT) describes how an abnormal focus within the composite homunculus can be set up as the equivalent to a peripheral disease process. But how can modern medicine be the beneficiary of such a concept? In theory if the neurons associated with the centrally located pathological neural circuitry can be manipulated or modulated to get rid of their abnormal activities, then homeostasis in the periphery can be reestablished and the process of disease eliminated. In practice, brain stimulation such as surgical implantation of electrodes on the periaqueductal grey and the sensory thalamus has also been used to treat intractable pain (29). Though clinical success has been reported, the expense, mortality and morbidity associated with the procedure prevented it from being a commonly used method. Fortunately, the body of knowledge available in traditional Chinese medicine has provided modern clinicians with a simple way to manipulate the circuitries within the brain without cracking open the skull. According to TNT, the acupuncture points, the meridians and the intricate relationships they bear to one another constitute a road map that illustrates physiological dysfunctions within the CNS and the ways to manipulate them. In other words, nerve endings and receptors at specific anatomical locations easily accessible are used as switches to reprogram (to normalize) the malfunctioning neural circuitries in the brain. Clinical experience has led the author to realize the following important principles are at work:
Neural normalization by physical stimulation
An abnormal neuron with either a high or low level of excitability tends to become normoactive upon stimulation. In other words, an identical stimulation can produce opposite effects on a neuron depending on its beginning level of excitability prior to stimulation. The therapeutic efficacy of acupuncture is based on its normalizing effect on the abnormal neuronal focus within the composite homunculus. For example, the acupuncture locus known as Reflow (or Fu-Liu) of the kidney meridian can be stimulated to treat both hyperhidrosis (excessive sweating) and anhidrosis (excessive dryness) of the hands, conditions on both ends of the same physiological spectrum.
Principles of repetition
The normalization effect of physical neuromodulation is often transient, providing only temporary relief of symptoms. Therapies therefore must be given at frequent intervals in order for the normalization to take hold to effectuate a permanent cure; This process, called reversed habituation, dehabituation, or new habituation, involves the same learning process for the neurons as the origination of the pathological process except in an opposite direction. Parallel to the pathological habituation process, a single powerful stimulation delivered at the abnormal neural circuit can sometimes accomplish the same result as a series of milder stimulations, much like a single overwhelming noxious insult can habituate a neural circuit into dysfunction.
Principle of contiguity
The normalizing process of neurons is 'contagious'. In other words, normalization of a neuron tends to normalize the neighboring neurons, presumably due to its synaptic connections with the surrounding neurons. According to TNT, the reason why an acupuncture locus is super-effective in the treatment of disease is due to the extensive network of connections possessed by the neuronal clusters in the composite homunculus representing the acupuncture loci in the periphery. Furthermore, individual neurons belonging to the same neuronal chain can be considered as physically contiguous because of the facilitated transmission along such a pathway which is equivalent to a meridian. Hence, it is consistent with the teaching in classical acupuncture that any point on the meridian can be used to treat disease processes affecting that meridian, as the normalizing impulse from such an acupuncture point can spread along the entire chain of neurons
Anatomical parts that seem to be far apart are often represented by neurons physically close together in the homunculus as outlined under principle II. For example, the Grand Convergence point (Bad Huey) on the vertex of the head is used to treat conditions around the anal area including hemorrhoids because the embryonic scheme of TNT places the head deep into the pelvic region. The lack of physical barrier within the homunculus permits the spread of influence from one body area to another much more easily in the brain than in the periphery. This viewpoint is supported by observations in a great many situations in the modern medical setting. For instance, skin rashes associated with viral infections follow either a centrifugal (spreading from the trunk towards the head and extremities) or centripetal (beginning from extremities and spread towards the trunk) distribution. Examining the homunculus model of TNT, it would not be difficult to realize if the pathological focus begins at the pole near the head and extremities and spreads towards the opposite pole, the centripetal pattern would result as in erythema multiforme and small pox (30). Conversely, if the focus begins from the other polar region close to the back and works its way towards the head and extremities, the skin rash would follow a centrifugal pattern as in urticaria (31). A pathology below the diaphragm such as cancer of the liver can induce pleural effusion above the diaphragm (32), and the so-called double effusions (pleural and peritoneal effusions) are found in dogs and cats with non-neoplastic liver diseases and pancreatitis (33), as the barrier of the diaphragm does not exist in the composite homunculus within the brain, so the neurons composing the abnormal focus representing the liver or pancreas can have negative influence on the neighboring neurons representing the lower thorax.
Principle of catharsis or healing crisis
During the neuronal normalization process, especially from a hyperexcitable state, it is not uncommon to observe transient but highly noticeable aggravation of symptoms, followed by recovery. Pathogenic biochemical substances within the neurons that cause symptoms upon their intermittent releases may be unloaded at once in the process of normalization, resulting in an apparent flairup. However, once the 'pathological content' has been unloaded, the neuron regains its normal function and symptoms no longer recur. The term catharsis, in its normal usage in psychiatry, may in fact be the unloading of an overcharged emotional neural circuitry. Not surprisingly, cathartic reactions, also known as healing crisis are frequently encountered in acupuncture and Chinese herbal therapy as well as homeopathy, as all such therapies effectuate the cure by acting on the composite homunculus in the CNS, as shall be further discussed under the principle of dehabituation.
The principle of chemo-neuromodulation
If physical stimulations applied to the peripheral nerve endings such as those at the acupuncture points can modulate neural circuitries within the CNS via the composite homunculus as proposed in TNT, the next logical question is whether chemical substances applied to the same peripheral receptors can also achieve central neuromodulations. Here the chemical substances do not merely act as irritants but as chemical stimulants with high degree of specificity recognizable by the CNS. The arguments and evidence in support of this principle are many-fold:
CNS sensing of the peripheral chemical environment
According to TNT, the CNS controls all peripheral physiological functions. In order to do so, it must receive incoming information concerning the peripheral chemical as well as physical environment. And how else would it be able to sense the chemical environment unless chemical messages can be transmitted from the peripheral nerve endings and receptors afferently to the brain, or more specifically, to the composite homunculus. Furthermore, these incoming chemical signals must first affect the central neural circuitries in some way to induce a CNS response of sending out the necessary commands to the periphery to maintain its homeostasis. Therefore principle I, namely, the general CNS principle necessitates the logical conclusion that chemical messages emanating from the periphery can indeed be transmitted to the representing neurons in the brain to affect their circuitries. Chemical manipulation of the CNS by applying chemical stimulations at the periphery can therefore be properly termed chemo-neuromodulation.
Chemical transport from peripheral to central nervous system
In order for the periphery which sends in the chemical messages to influence its counterpart in the composite homunculus, the chemical substance itself or a transduced chemical messenger on its behalf must be able to travel afferently along the same pathway as a CNS-bound physical stimulation. A retrograde transport system must exist along the peripheral nerve and up the spinal cord before reaching the composite homunculus system. Molecular messengers must also be able to migrate across the synapses. This type of retrograde transport system has been found to exist. For example, substance P. a small peptide, has been shown to accumulate, after ligation of the dosed roots, on the peripheral side of the ligation and also decrease dramatically in the intermediate neurons in the substantia gelatinosa in the spinal cord (34). This demonstrates clearly that such a substance is transported afferently and across a synapse. A fast axonal transport system for organelles carrying various molecules in both anterograde and retrograde directions has also been shown to be present in mammalian (rat) nerves. Certain synapsins are known to be bound to these transported organelles (35,36). And Herpes Simplex virus can travel from the periphery to the brain by axonal transport within the neurons and can be selectively transferred across synapses (37). Dopamine transporter is also known to be bound to a variety of drugs (38). Summing up observations such as these and others, it is quite clear that pharmacological agents can in fact travel from peripheral nerve endings to the CNS to exert their chemo-neuromodulation effects.
Evidence of chemo-neuromodulation in Chinese medicine
According to TNT, homeopathic remedies and traditional Chinese medicine, i.e. herbal therapies and acupuncture are based on knowledge of the CNS network, which is being utilized to modulate and normalize the abnormal circuitries within the CNS via physical or chemical means. Consider the following examples:
-
Application of the powder of Fructus Evodiae mixed with rice vinegar or Yung-Chuan (surging spring) point, the first point of the kidney meridian at the bottom of the foot to treat furuncle located right next to the nostril (39).
-
Application of a paste made from the ground powder of Radix Boehmeriae on the tip of the big toe to treat scrotal pain on the contralateral side (39).
-
Application of Semen Ricini to Bai Huey point on the vertex of the head to treat prolapse of the uterus (39).
-
Application of minute amount of finely powdered borax to the corners of the eyes to induce tearing for the treatment of acute back sprain (39)
Obviously, the common denominator of the above treatments is the application of a pharmacological agent at a site bearing no peripheral anatomical relationship whatsoever with the pathological focus except the point of treatment and the site of pathology are indeed next door neighbors within the CNS according to the composite homunculus plan proposed in TNT. Consequently, chemo-neuromodulation at the treatment point can normalize in the CNS the abnormal neurons representing the diseased part (Principle V.3).
By far the most common neuromodulation modality in traditional Chinese medicine is moxibustion -the burning of moxa (Artemisia vulgaris) to generate heat at acupuncture loci to treat diseases. Moxa instead of other heat source such as a burning incense is used by reason of its medicinal property of moving chi in the body as it is also prescribed as an oral medicine for other maladies of 'stagnant chi'. Its chemical actions at the acupuncture point must be significant and can be appropriately considered a form of chemo-neuromodulation, in addition to being a form of physical neuromodulation.
Many Chinese herbal agents can be taken internally and applied externally for the treatment of diseases. While only a minute amount of medicine can be absorbed at an acupuncture point, its effectiveness depends on its specific chemo-neuromodulation of the CNS. The same medicine, taken internally in much larger quantities, according to TNT, must also act on the same central neural circuitries to achieve its therapeutic effects. In this latter scenario, the pharmacological molecules either modulate the CNS directly or indirectly by (1) crossing the blood-brain barrier, (2) by travelling afferently via neuronal transport or (3) by first acting on a cellar component in the periphery, producing chemical changes that can be transduced by the peripheral nerve endings which are ubiquitous in various parts of the body, into chemical or physical messages, which in turn act on and modulate the CNS.
This chemo-neuromodulation concept, along with the other principles outlined above is presumed to be the foundation of traditional Chinese medicine and homeopathy. Since the intricate networks within the CNS are still poorly understood today, the clinical phenomena observed in the practice of traditional Chinese medicine and homeopathy cannot be explained on the basis of present knowledge in modern Western medicine. Light, however, can be shed on the efficacy of these treatments by TNT as illustrated in subsequent sections of this article.
Principle of dehabituation or principle of adynamic stat
(principle of the stuck switch)
According to the present hypothesis, sickness is the result of pathological habituation of a neural circuitry within the composite homunculus, which can be normalized by repetitious stimuli, or a single or several powerful stimuli. These dehabituatingneural inputs come in many forms:
Interruption of stimulation as a form of stimulation. In modern medicine, local anesthetics have been injected into trigger points to treat chronic myofascial pain. The resulting pain relief often lasts much longer than the duration of action of the anesthetics, and repeated injections may even eliminate the pain permanently. This clinical phenomenon cannot be explained by the physiology of the peripheral nervous system alone. In accordance with TNT, trigger points which often coincide anatomically with acupuncture loci, are merely the peripheral corresponding counterparts of the hyperexcitable neurons within the central homunculus. Normally, there is a stream of neurosensory input flowing from the trigger point to the focal hyperexcitable neurons in the homunculus. The constant neuronal firings at the periphery are temporarily interrupted by the local anesthetic. This sudden cessation of neural input is perceived by the hyperactive central neurons as a form of stimulation. In response to the stimulation, they normalize and pain relief is achieved. Once normalization is induced, it can outlast the duration of the inducing stimulation, in this case the duration of pharmacological action of the local anesthetic.
Paradoxical normalization - shifting control away from normal position to normalize The exact therapeutic mechanism of homeopathy has remained a puzzle, although the basic rules governing this type of therapy are rather straight forward.
Rule A. Homeo means similar and pathy means treatment. Homeopathy is
based on the concept of using substances to reproduce existing symptoms
to trigger healing.
Rule B. Very minute doses of substances are used.
Rule C.Existing symptoms often exacerbate to an extent far exceeding what is to be expected from the minute dose of medicine which technically may be considered a toxin.
These observations can be interpreted in the light of TNT quite readily.
Since the symptoms of an illness depend on which part of the composite homunculus the pathological focus resides in, a homeopathic dose that duplicates or mimics the exact symptoms are likely to act on the same deranged neural circuitry. In other words, the selection of the medicine ensures this form of chemoneuromodulation is directed solely towards the exact abnormal focus within the CNS.
As the symptoms of the disease result from the physiological stat being set outside of the normal range, stimulating the abnormal neurons composing this control tends to set them straight (see Principle V-l.). In this instance, the stimulation is accomplished by pushing such a physiological stat further away from the normal position. Theoretically, the extremely tiny amount of homeopathic dose should make the symptoms a little worse. In practice the 'infinitesimal' worsening of the condition often leads toremission of symptoms and cure of the sickness, as if giving the switch controlling the symptoms an extremely gentle push further away from normal ever so slightly allows it to bounce back into the normal range.
As treatment progresses, old symptoms seem to exacerbate, much like the phenomenon of healing crisis associated with acupuncture treatments, which, of course, also act on the CNS.
Normalization by normalizing. This principle is typified by traditional Chinese medical therapy. So if the system is too 'hot' (hypermetabolic), the treatment is to cool it (reduce metabolic activities); too cold, warm it. If the system is too congested (hyperexcitable), drain its energy (reduce excitability); too deficient, strengthen it, and so on down the line. The password here is normalization. The central neuronal circuitry controlling the heart rate, if set too high, causes palpitations; too low, syncope (from slow heart rate). Similarly, if neurons comprising the circuitry controlling intestinal motility is overly active, abdominal cramps ensue. Conversely, a low motility-stat leads to symptoms of indigestion, constipation, ileus, etc. Accordingly, a typical Chinese medicinal concoction is made up of a number of ingredients working in concert to normalize the disease process. Well established ancient formulae, upon careful analysis with the current theory are shown to contain but a few basic rules:
-
Therapeutic agents to activate the meridians or segments of meridians containing the disturbances, setting them up for modulation by companion drugs.
-
Therapeutic components as companion drugs to rectify the focal abnormality, which may be too hot (hypermetabolic), cold (hypometabolic), congested (over-reactive), deficient (underreactive), wet (hypersecretory) or dry (hyposecretory), etc.
The prime purpose is to get rid of the blockage and reestablish the flow of chit If the symptoms are due to pathological habituation with the controlling switch set too high or too low, much like a switch stuck at the wrong position, the treatment policy is to push or pull the stuck switch back into the normal range.
Normalization by combination of normalization and paradoxical normalization Sun Se Miew, a renowned Chinese physician in the sixth and seventh centuries (581 - 682 A.D.) was himself utterly baffled by the efficacy of a well proven formula, Yuan Hua Powder, composed of pharmacological agents of seemingly opposite therapeutic effects, namely, hot and cold agents used in the same formula (40). The puzzle remains unsolved today, as no satisfactory explanation has been advanced. Using the current model, however, such a dilemma can be easily overcome. If either homeopathy, which works by pushing the controlling switch further away from normal, or Chinese medicine, which works by pulling the switch towards normal, alone can attain a cure by stimulating and thus normalizing the abnormal neuronal circuitry, why not combine the two modes of therapy for greater efficacy? In fact, quite a few proven Chinese herbal formulae already contain therapeutic agents of opposing effects. Like a window stuck at a certain position cannot be pushed open at first, but can do so after being pulled first and then pushed. The author nick-named this phenomenon the Stuck Switch Principle. The 'wriggling' provided by the opposing pharmacological agents may somehow loosen the switch, causing it to drift back to the normal position.
If the CNS is simply viewed as the substrate on which Chinese medicine and homeopathy act, then the cloak of mystery of these unconventional treatments could be shed instantly, although the cellular and molecular mechanisms accounting for the phenomenon remains to be elucidated.
Principle of chemo-immuno-neuro-endocrino-modulation
Traditional Chinese medicine categorizes Chi into defensive chi and nutritional (metabolic) chit Defensive chi naturally has something to do with warding off pathological processes including exogenous noxious stimuli such as infections. This partnership forged between chi and the body's defense system signifies the inseparable relationship between the nervous system and the immune system in today's terms. This seemingly ancient concept in fact embodies the prevailing thinking in the biomedical circles today. It has been found that the central and peripheral nervous systems, the endocrine and immune systems are extensively integrated with the boundaries defin-ing such systems both anatomically and molecularly blurred (41). The evidence is eloquently summarized by Home-Delarche and Dardenne (42):
-
The neuroendocrine system is able to modulate the immune response and the immune system can also function as a neuroendocrine organ, since it can synthesize not only hormones and neural peptides, but also cytokines.
-
The existence of cytokine receptors in the CNS and various cytokine effects on the CNS including neuromodulatory actions, fever induction, sleep and food intake functions have been demonstrated.
-
Demonstration of cytokine production by CNS cells and all phases of immune response can potentially occur within the confines of the blood-brain barrrier.
Additionally, other known neuroendocrine molecules such as catecholamines can be immune suppressive and they can inhibit lymphocyte activation (43). The phenomenon demonstrates the bi-directional interactions between the nervous and immune systems (44). Furthermore, molecules which play important roles in the nervous system share a close structural similarity with those of interleukin-6 which is a molecule acting on the immune system. And molecules regulating the neural development and those acting in the immune system have a common evolutionary origin (45).
In view of the compelling evidence, it is the author's opinion that the immune system should be viewed as a mobile component of the portion of the CNS that specializes in defense functions, which is the stationary component. Though capable of receiving information from and sending out chemical messages to the periphery relatively quickly, the nervous system is after all stationary and so must rely on rapidly mobile vehicles such as blood and lymph that can travel through the vascular beds and lymphatic vessels speedily to the sites of injury, invading infective agents or foreign matters.
Theoretically, any link along this chemo-neuro-immuno-endocrinal axis can be used to modulate the other components. As a wide spectrum of factors and receptors such as neuro-tropic factors, cytokines including prostaglandins, interleukins and neural peptides are found both in the CNS, the periphery and the immune system, these may all be considered the alphabets or communicating tools for these different physiological compartments. As such they can be used to modulate the CNS effectively to cure diseases. A handful of well known clinical examples are worth mentioning:
-
Transplantation of adrenal medullary tissue into the spinal subarachnoid space is highly effective in controlling chronic pain (46).
-
Surgical implantation of fetal tissue in the brain to treat Parkinson's disease (47).
-
Intramuscular injection of sheep fetal cells has been used in Europe as a rejuvenation therapy which allegedly produces marked revitalization of the body's functions, including sexual functions
The single common denominator shared by these treatment methods is the usage of tissues rich in neural factors. Likewise, molecular products derived from the immune system such as those from macrophages have also been shown to modulate the nervous system and can be used potentially to modulate the CNS to reestablish homeostasis. The neuro-neuromodulation (using neuropeptides) and the immuno-neuromodulation (using immune products) can be regarded as a specialized form of chemo-neuromodulation. The clinical implications of this concept will be further discussed in the last section of this article.
Principle of bilaterality
The periphery and CNS functions as an integrated whole, each influencing the other by constant physical and chemical communications and modulations. Rhythmic and sequential neuronal discharges and transmissions along the neuronal chains equivalent to the meridians not only provide a viable explanation of an internal clock, but such rhythmic neuronal activities may be involved in the control of the respiratory apparatus which includes the lungs, diaphragm, thorax, intercostal muscles, etc. When this internal driving force based on neural transmissions activates the peripheral neuro-muscular elements to consummate the act of breathing, these same elements, when voluntarily activated, also stimulate the neural circuitry controlling respiration. Chi-kung, a practice originating from ancient China involving rhythmic breathing and meditation along with mental imagery has been found to have significant health benefits. Tai Chi, a Taoist form of shadow boxing, adding body movements onto the equation, is also designated to strengthen and mobilize the chit From the viewpoint of TNT, the peripherally originated stimulations from the breathing apparatus, together with the imagery-induced, neocortex-originated stimulations on the composite homunculus, stimulate the respiration related neural circuitries and drive the chi or neural transmissions along these channels, normalizing and strengthening the neuronal functions along the way to maintain harmony or homeostasis for the entire body. Simply put, internal chi drives respiration and respiration drives internal chi
Exercise in general which projects a barrage of neural input to the CNS, though in a less concerted manner than chi-kung, is also well known to have health promoting effects. However, overly vigorous exercises, as in certain sports and aerobic exercises, can dissipate chi or neural energy quickly and the result may be harmful, for excessive firings may overwork the central neurons, causing a depletion of essential neural transmitters and modulators, leading to a state of exhaustion and deficiency. In extreme cases, This may even lead to chronic fatigue syndrome.
Neurons within the CNS must be stimulated in order to be healthy. Disuse atrophy from immobility is a prime example. The early mobilization of a patient after a major surgical operation is to stimulate the CNS (or mobilize the chi) to facilitate healing and early recovery. Crossed eyes in a small child, if not corrected, can cause loss of vision (amblyopia) in the 'lazy eye' for central neural connections cannot be made if they are not stimulated early in life (48). Sensory deprivation experiments further point to the fact that the absence of peripheral stimuli can cause severe disturbances in the CNS such as disorientation or even delusions and visual hallucinations (49). In Leber's congenital amaurosis, psychomotor retardation is thought to be the result of sensory deprivation (50). All these facts support the contention that bidirectional communications and stimulations are essential for maintaining homeostasis - a synonym for health.
Discussion, inferences, proposals and predictions
Revised concept of diseases
For example, both diabetes mellitus and Graves' disease (hyperthyroidism) can be viewed as diseases of the CNS with peripheral manifestations, each involving one primary target endocrine organ, namely the pancreas and the thyroid respectively. Little wonder the treatment of insulin-dependent diabetes with insulin can often only control the symptoms without the definite ability to prevent certain complications, such as retinopathy despite good blood sugar control (51). Diabetes is really a CNS disease affecting multiple organ systems even though many important symptoms are associated with the lack of insulin from the pancreas.
Graves' disease can be treated by destroying part of the thyroid gland with radioactive iodine but sornetimes exophthalmos (protrusion of the eyes), another prominent symptom of hyperthyroidism, continues to progress despite a normal functioning thyroid gland following treatment (52).
In both diseases, the endocrine dysfunction is only part of, albeit an important part of the total clinical picture, as the replacement of insulin or the destruction of the thyroid gland does not necessarily normalize the pathological neural circuitries within the CNS and the diseases progress to affect other target tissues and organs. The onset of insulin-dependent diabetes in children in not uncommonly preceded by an episode of infection such as mumps (16) and the onset of Graves' disease is often preceded by major emotional crisis or traumatic experience (54). In both cases, the CNS is involved according to the present theory, and the controlling neural circuitries are shocked into disarray, perpetuating the pathological processes. Comatose state as in a 'human vegetable', nerve deafness resulting from streptomycin toxicity, aplastic anemia as a result of bone marrow suppression by the antibiotic Chloramphenicol, catatonia from viral encephalitis, etc. may all be the result of neurophysiological shocks or rapid pathological habituations, and are therefore potentially reversible if the proper dehabituation treatments are instituted.
Old observations, new interpretations
Some individuals suffering from angina experience significant relief by undergoing thoracotomy but without heart surgery. According to TNT, thoracotomy gives rise to a powerful stimulation to the neurons representing the chest wall in the homunculus which then stimulate the hyperexcitable, symptom causing neighboring neurons representing the heart to normalize, resulting in relief.
The same neurophysiological scenario, to a lesser degree, takes place when local anesthetic is injected to the tender spots (trigger points) on the outside of the chest to stop anginal pain originating from the heart.
The symptom of shortness of breath is considered to be a highly subjective sensation from the modern medical viewpoint. The degree of severity of the symptom often is not proportional to demonstrable pathology in the respiratory system. According to TNT, the sensation of being short of breath is equivalent to a weak or impeded neural transmission (a weak or congested circulation of chi) along the neuronal pathway representing the lung system within the composite homunculus. Such an inefficient neural transmission can often be aggravated by exertion which puts additional demand on the system, making it more deficient in its transmission capacity. That is why a debilitated person gets out of breath upon minimal exertion.
Old methods, new applications
Repetitious nerve blocks to treat chronic pain. Neural destructive techniques such as rhizotomy, cingulotomy, neurectomy, thalamotomy, etc. have been found to be only temporarily effective (55-57), producing pain relief lasting several weeks to several months. The failure of these methods is due to the lack of repetition, for once the nervous tissue is destroyed, the treatment cannot be reinstituted. The pathological focus representing pain must be dehabituated or must re-learn to be normal and that takes repeated training. The severing of a nerve tract intercepts peripheral stimulation, much like what a nerve block does. Nerve blocks, unlike the destructive techniques, however, can be repeated over and over again. Again according to TNT, if a nerve block is successful in providing temporary and complete pain relief, it signifies that the neurons in the abnormal central circuitry have been effectively stimulated. All one needs to do now is to keep on repeating the same in sufficient frequency such as every other day or every 2-3 days for a series of 10-12 treatments. And if necessary, more than one series of treatments can be given. Permanent pain relief can often be attained this way.
Multiple surgeries for metastatic cancer. If repetitious stimulations is the key in the treatment of chronic diseases, might cancer that has spread be treated the same way? According to TNT, a pathological neuronal focus must simultaneously exist in the brain as the cancer cells in the periphery. The therapeutic objective would be to convert these neurons of abnormal activities back to normal in order that peripheral homeostasis be reestablished. Surgery which involves cutting and removal of tissues, in and by itself is a strong stimulation. A cancer is considered inoperable if it has spread diffusely and all of the cancer cells cannot be surgically removed. However, the complete removal of all the cancer cells at once may not be necessary in order for the patient to benefit from the procedure from the TNT's view-point. As each discrete mass of tumor is removed, a strong stimulation is delivered to the abnormal focus within the composite homunculus to initiate a normalizing trend. But if permanent benefit is to be obtained, surgery must be repeated with additional cancerous tissues removed each time to dehabituate and normalize the abnormal focus on a long term basis. From the viewpoint of Chinese medicine, cancer of the congested rather than the deficient type should be more amenable to this approach. Concurrent with the series of operations, the body should be fortified by other adjunctive therapies such as Chinese herbal medicine, acupuncture, or other innovative treatments to be described in subsequent sections.
Combining Chinese medicine and homeopathy
TNT presumes the stuck switch phenomenon (pathological habituation) exists in all chronic conditions and since homeopathy is geared to pushing the switch away from the normal position, whereas Chinese medicine is effective in pulling that same switch towards the normal position, combining the two disciplines will have the effect of pushing and pulling that same switch, getting it unstuck from its pathological position and allowing it to return to normal, thus effecting a cure. This strategy has not been attempted clinically but is well worth trying.
Therapies of specificity
More often than not, currently available therapies lack specificities, as they do not focus exclusively on the pathological neural circuitries themselves. With the exception of acupuncture therapeutics, this statement holds true for modern medicine and partially true for Chinese medicine and homeopathy. The pharmacological dose is usually delivered orally or parenterally to the entire body so only those drug molecules that act on the tissues that relate to the specific abnormal neural circuitries are exerting their maximum therapeutic effects. Most of the dose that acts on irrelevant tissues is either wasted or producing side effects. Higher dosages may be more effective but are more likely to cause untoward reactions and/or toxicities. Based on the principles of TNT, if the therapeutic chemical substances can be delivered in a way to act specifically and exclusively on the malfunctional neural circuitry, then it would be equivalent to a therapeutic dosage many times higher than can be safely administered systemically, powerful enough maybe to treat the more chronic and intractable problems. Fortunately, the system of meridians and acupuncture points permits precise access to the deranged neural circuitry in the brain readily so a much smaller quantity of medicine than an oral dose can be delivered specifically to these loci to elicit a much more dramatic overall clinical response.
The line of reasoning goes like this:
-
Stimulation at properly selected acupuncture points will reach and modulate the pathological focus in the CNS
-
The effectiveness of Chinese medical agent, taken orally, is based on its ability to directly or indirectly chemo-neuromodulate the central neural circuitry controlling the disease process. So there is a chemical linkage between the therapeutic molecule and the neuronal function. But this method is wasteful and lacks specificity
-
Despite its very small quantity, the same medical agent delivered to specific peripheral nerve endings at the acupuncture points will specifically chemo-neuromodulate the abnormal focus in the CNS effectively without adverse reactions.
Linking up with modern technology
Unavailable to the most sophisticated Chinese physicians centuries ago, the hypodermic needle and syringe is indeed a high-tech instrument for neuromodulating substances to be delivered at specific acupuncture points. In addition to traditional Chinese herb agents, a wide variety of pharmacological agents including neurotrophic factors, cytokines, products from the immune cells, etc. can potentially be used specifically to modulate the focal pathological cir-cuitries within the composite homunculus. Besides injecting acupuncture points, endoscopy, colonoscopy, bronchoscopy, laparoscopy, etc., are but a few of the techniques available to access various parts of the interior of the body to implement the.chemo-immuno-endocrino-neuromodulation therapy. In China, implantation of special sutures at acupuncture points has been used to treat neoplastic diseases (58) and in-jection of bee venom at acupuncture points has been used to treat arthritis. These treatment methods are perfectly consistent with the principles outlined in the present theory.
Predications based on TNT
Experimental confirmation of TNT. To verify TNT, a mini brain, a nucleus or structure organized in the same architectural plan as the curled up embryo proposed by the theory must be discovered. The most logical place to look for such a structure should be phylogenetically the oldest part of the brain. It should be pointed out, however, duplicate plans may exist in more than one location within the CNS, as such a redundant system affords greater protection to the organism should something happen to the master homunculus. After the mini-master brain is identified, its connections to other portions of the brain should be traced. Since embryological development is a recapitulation of past evolutionary events, phylogenetically the older part of the brain represents the central nervous system of an earlier life form in the human ancestry. The master homunculus, organized as an embryo, may in fact embody the blue print of somatic development. If so, this master mini-brain should also be already present in early embryological development, as it should be found in the oldest part of the CNS. As new and more advanced species emerged in the course of evolution, additional CNS functions as well as additional portions of the brain were added onto this primordial nervous system. According to this scheme, the newer parts of the brain really grow out like branches of a tree from the primordial brain which behaves as if it is the root. The master homunculus may be connected to similarly old homunculi which in turn make connections with the rest of the brain. Consequently, as various parts of the brain ultimately make direct or indirect connections with this primordial brain containing the master homunculus, the whole CNS behaves like a composite homunculus. Evidence to support this theory include similarity between the embryonic cleavage planes and the distribution of the meridians. If the master homunculus indeed directs the embryonic development of the entire body, it is only logical that it retains control over the entire body. It should be pointed out that the master homunculus may be quite small anatomically, and due to the large size of the head and extremities and its folded posture, anatomical localization for neurons representing various parts of the body may be grossly distorted spatially, especially if the investigator is not aware of this particular architectural plan. Embryological development should also be treated according to this reference system to see if the pieces of the jigsaw puzzle fit.
Symmetry of neural factors. Since a great variety of trophic factors controlling differentiation and directions of development are present during the embryonic stage, many such factors may still be present in the adult brain, some remaining active and others under suppression. As CNS is the master control of the body, bilateral communication between the CNS and the periphery is a must and this requirement necessitates the use of chemical dialogues mediated by various types of peptides, trophic factors, cytokines, etc. Several of these factors such as prostaglandins and endorphins were first discovered in peripheral tissues and later on in the CNS (59,60). As the current hypothesis emphasizes on symmetry and bilaterality, one should expect to find many, if not all of such substances at both the central and peripheral locations, even though some may be found so far in only one.
Immuno-neural convergence. The immune and nervous systems in TNT's view are not just linked but in fact merged as one system. Neuronal memory and immunological memory may have a very similar physiological basis. Since immunological memory does not easily fade away, that memory must be stored at some place other than a mobile cellular compartment (such as the immune cells) with limited life span. A stationary memory system to encode past immunological events ought to exist as in the case of ordinary memory. Therefore, stationary organs such as the thymus could be logical candidates. The central nervous system itself may even be a storage site for immune memories. This conjecture remains to be explored.
While the Thalamic Neuron Theory needs to be correlated with actual cellular and biochemical events, it remains a useful model to logically explain various forms of healing such as Chinese medicine and other alternative therapies, so that their seemingly abstruse principles no longer appear esoteric and mystical. These very same principles can also account for the many clinical phenomena observed in modern Western medicine but which defy explanation by present 'modern' medical knowledge. This is so because our current knowledge of the intricacies and complexities of the networking within the central nervous system is at best primitive. Clinical applications based on the Thalamic Neuron Theory, if successful, should further lend support to its validity and if the theory is proven correct at the cellular and molecular levels, it should prompt a major revolution in medicine, with the merging of all medical disciplines, allopathic and homeopathic, Eastern and Western, modern and ancient, ushering in a new era of medicine using an endless array of new treatment modalities.
REFERENCES
-
Lee TN. Thalamic Neuron Theory: A hypothesis
concerning pain and acupuncture. Med Hypotheses 1977; 3:113-121.
-
Hassler R. Afferent Systems. Pain. Baltimore,
Maryland: Williams and Wilkins.
-
Lee TN. A treatise on acupuncture meridians.
Am J Acupuncture 1978; 6:283-288.
-
Lee TN. The thalamic neuron theory and
classical acupuncture. Am J Acupuncture 1978; 6:273-282.
-
Lee TN. Thalamic neuron theory, the
law of the five elements and the rhythmic method of classical acupuncture.
Am J Acupuncture 1981; 9:217-226.
-
Hsu Sik Lian et al. Rhythmic method
of acupuncture. Hong Kong: Nan Kwong Publishing.
-
Pavlov IP. The scientific investigation
of psychical faculties or processes in the higher animals. Science 1906;
24:613-619.
-
Kandel ER. Nerve cells and behavior.
Sci Amer 1970; 233:5767.
-
Rempel DM, Harrison RJ, Barnhart S.
Work-related cumulative trauma disorders of the upper extremity. JAMA 1992;
267:838-842.
-
Benson H. Herd JA, Morse WH, Kelleher
RT. Behaviorally induced hypertension in the squirrel monkey. Circ Res
1970; (1 Suppl 1): 21-26.
-
Herd JA, Morse WH, Kelleher RT, Jones
LG. Arterial hypertension in the squirrel monkey during behavioral experiments.
Am J Physiol 1969; 217:24-29.
-
Dahl LK. Salt and hypertension. Am J
Clin Nutr 1972; 25:231 -244.
-
Frohlich ED, Chien Y. Sesoko S. Pegram
BL. Relationship between dietary sodium intake, hemodynamics, and cardiac
massin SHR and WKY rats. Am J Physiol 1993; 264(1 Pt 2):R30-34.
-
Femandez A, Hontebeyrie M, Said G. Autonomic
neuropathy and immunological abnormalities in Chagas' disease. Clinical
Autonomic Research 1992; 2(6):409-412.
-
Schroeder SA, Krupp MA, Tiemey Jr LM.
Current Medical Diagnosis and Treatment. Appleton and Lange, 1988: 196,536.
-
Sultz HA, Sdao M. Mumps and childhood
diabetes: epidemi- 37. Ology and disease causation. Compr Ther 1975; 1:68-72.
-
Forrest JM, Menser MA, Burgess JA. High
frequency of dia- 38. betes mellitus in young adults with congential rubella.
Lancet 1971; 2(720):332-334.
-
Beijing Chinese Medica! College. The
Grand Thesis of the 39. Phenomena of Yin and Yang. In: Textbook on Nei
Ching. Hong Kong: Medical and Health Publishing, 1978.
-
Rosenfeld JP. Applied psychophysiology
biofeedback of event-related potentials (brain waves): historical perspective,
review, future directions. Biofeedback Self Regul 1990; 15:99119.
-
Weil A. The Natural Mind. Boston: Houghton
Mittlin, 1972.
-
Waters TA. Psychologistics: an Operating
Manual for the Mind. New York: Randon House, 1971: 31.
-
Murison R. Overmier JB. Some psychosomatic
causal factors of restraint-in-water stress ulcers. Physiol Behav 1993;
53(3):577-581.
-
Gutstein WH, Harrison J. Parl F. Ku
G. Avtable M. Neural factors contribute to atherogenesis. Science 1978;
199:449-451.
-
Kaufman HH, Timberlake G. Voelker J.
Pait TG. Medical complications of head injury. Med Clin North Am 1993;
77:43-60.
-
Owman C. Peptidergic vasodilator nerves
in the peripheral circulation and in the vascular beds of the heart and
brain. Blood Vessels 1990, 27:73-93.
-
Charnley RM, Thomas WM, Stanley J. Morris
DL. Serum gastrin concentrations in colorectal cancer patients. Ann R Coll
Surg Engl 1992; 74:138-140; discussion 141.
-
Talmi YP, Hoffman HT, McCabe BF. Syndrome
of inappropriate secretion of arginine vasopressin in patients with cancer
of the head and neck. Ann Otol Rhinol Laryngol 1992; 101 :946-949.
-
Warrell RP Jr. Etiology and current
management of cancerrelated hypercalcemia. Oncology 1992; 6:37-43, discussion
43, 47-50.
-
Hosobuchi Y. Combined electrical stimulation
of the periaqueductal gray matter and sensory thalamus. Appl Neurophysiol
1983; 46:112-115.
-
Lewis, GM, Wheeler Jr CE. Practical
Dermatology, 3rd edn. WB Saunders Company, 1967: 151,341.
-
Lewis, GM, Wheeler Jr CE. Rractical
Dermatology, 3rd edn. WB Saunders Company, 1967: 147.
-
Spizemy DL, Gross BH, McLoud T. Enlarging
pleural effusion after liver transplantation. I Thorac Imaging 1993; 8:8587.
-
Steyn PF, Wittum TE. Radiographic, epidemiologic,
and clinical aspects of simultaneous pleural and peritoneal effusions in
dogs and cats: 48 cases (1982-1991). J Am Vet Med Assoc 1993; 202:307-312.
-
Nicoll RA, Schenker C, Leeman SE. Substance
P as a transmitter candidate. Am Rev Neuro Sci 1980; 3:227-268.
-
Sheetz MP, Steuer ET, Schroer TA. The
mechanism and regulation of fast axonal transport. Trends Neurosci 1989;
12:474-478.
-
Dahlstrom AB, Czemik AJ, Li JY. Organelles
in fast axonal transport. What molecules do they carry in anterograde vs
retrograde directions, as observed in mammalian systems? Mol Neurobiol
1992; 6:157-177.
-
Breakefield XO, DeLuca NA. Herpes simplex
virus for gene delivery to neurons. New Biol 1991; 3:203-218.
-
Kuhar MJ, Sanchez-Roa PM, Wong DF et
al. Dopamine transporter: biochemistry, pharmacology and imaging. Eur Neurol
1990; 30 Suppl 1:15-20.
-
Huang T. External Treatment Methods
of Chinese Medicine. Medical Publisher of China, 1966: 8,20,28,45.
-
Chung Du Chinese Medical College. The
Theories of Different Schools in Chinese Medicine. Kwei Jo People's Publishing,
1988: 39.
-
Cash JM, Wilder RL. Neurobiology and
inflammatory arthritis. Bull Rheum Dis 1992; 41:1-3.
-
Homo-Delarche F. Dardenne M. The neuroendocrine-immune
axis. Springer Semin Immunopathol 1993; 14:221-238.
-
Chambers DA, Cohen RL, Perlman RL. Neuroimmune
modulation: signal transduction and catecholamines. Neurochem Intemational
1993; 22:95-110.
-
Yokoyama MM. Neuronal and immune interactions.
No To Hattatsu 1993; 25:114-121.
-
Yamamori T. Sarai A. Coevolution of
cytokine receptor families in the immune and nervous systems. Neurosci
Res 1992; 15:151-161.
-
Sagen J. Chromaffin cell transplants
for alleviation of chronic pain. Asaio 1992; 38:24-28.
-
Ahlskog JE. Cerebral transplantation
for Parkinson's disease: current progress and future prospects. Mayo Clin
Proc 1993; 68:578-591.
-
Magramm 1. Amblyopia: etiology, detection,
and treatment. Pediatrics in Review 1992; 13:7-14.
-
Kolb LC. The cause and nature of mental
disorders. Noyes' Modem Clinical Psychiatry. Philadelphia, London, Toronto:
WB Saunders Company, 1968: 130.
-
Nickel B, Hoyt CS. Leber's congenital
amaurosis. Is menlal retardation a frequent associated defect? Arch Ophthalmol
1982; 100:1089-1092.
-
Crabbe JC. Diabetic complications: scientific
and clinical aspects. Edinburgh, New York: Churchill Livingstone, 1987.
-
Beeson PB, McDermott W et al. Cecil-Loeb
Textbook of Medicine, 12th edn. WB Saunders Company, 1967: 1294.
-
Beeson, PB, McDermott W. et al. Cecil-Loeb
Textbook of Medicine, 12th edn. WB Saunders Company, 1967: 1289.
-
Loeser JD. Neurosurgical relief of chronic
pain. Postgrad Med 1973, 53:115-119.
-
Rosomoff HL. Neurosurgical control of
pain. Ann Rev Med 1969; 20:189-200.
-
Loeser JD. Dorsal rhizotomy for the
relief of chronic pain. J Neurosurg 1972; 36:745-750.
-
Health Dept. of Military Reserve of
Canton. Manual of Commonly Practiced New Therapeutics. Beijing: People's
Health Publishing Co., 1970.
-
Dray F, Wisner A, Bommelaer-Bayet MC
et al. Prostaglandin E2, leukotriene C4, and platelet-activating factor
receptor sites in the brain. Binding parameters and pharmacological studies.
Ann NY Acad Sci 1989, 559:100-111.
-
Hartwig AC. Peripheral beta-endorphin
and pain modulation. Anesth Progress 1991; 38:75-78.
|